Menu
Surgery is a common treatment for prostate cancer. Surgery is used to potentially cure the cancer by completely removing the tumour or to reduce urinary symptoms.
The type of surgery done depends mainly on the stage of the cancer and other factors, such as your age, general health, and life expectancy. Side effects of surgery depend on the type of surgical procedure.
Radical prostatectomy is the most common surgical procedure for treating localized, low-risk, intermediate-risk or high-risk prostate cancer. It is a major surgery offered to men in good health.
A radical prostatectomy is the total removal of your prostate and the surrounding tissues. It is done as a potential cure for prostate cancer as it removes all cancerous cells. It can be combined with other treatments—for example, surgery followed by radiation therapy if needed.
Sometimes prostate cancer with only microscopic spread to your lymph nodes can be cured with surgery. How do you know if your cancer has spread to your nodes? Thanks to modern investigative techniques, it is rare that we have to wait until the operation to realize that the cancer is too widespread to be able to perform a prostatectomy.
That being said, if your cancer is more aggressive and you choose to go with radical surgery, your surgeon will remove your major pelvic lymph node groups during the operation. It is not necessary to remove them if your cancer is at a low risk of progression.
Unlike radical prostatectomies where your prostate and its capsule are removed, a transurethral resection of your prostate (TURP) consists of removing the internal lining of your prostate through your urethra while leaving your prostate capsule in place. This is the most common surgical procedure for benign prostatic hyperplasia (BPH or enlarged prostate).
In general, transurethral resection of the prostate (TURP) is usually given to relieve urinary problems caused by a prostate that has increased in size and is compressing the urethra. It is also used as a palliative treatment to relieve urinary obstructions in patients with advanced prostate cancer who are not healthy enough to undergo radical surgery.
You may opt for this surgery:
A radical prostatectomy is effective in the early stages of cancer when it is still confined to your prostate. Chances for recovery are excellent and it offers a high probability for long-term survival (more than ten years).
 Techniques to surgically remove the prostate include open surgery, hand-assisted laparoscopic surgery and robot-assisted laparoscopic surgery.
Techniques to surgically remove the prostate include open surgery, hand-assisted laparoscopic surgery and robot-assisted laparoscopic surgery.
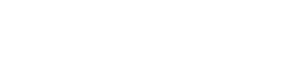
Traditionally, surgeons perform open radical prostatectomies through an incision in the lower abdomen (hence the term “open surgery”). This surgery allows for the removal of your pelvic lymph nodes before your prostate is removed.
Experienced surgeons are able to identify your erectile nerves and separate them from either side of your prostate in order to spare them from damage during the operation.
This operation is available in most hospital centres in Quebec and across Canada.
This nerve-sparing technique is not used by all surgeons since it is more complicated and delicate than the traditional method. You should speak to your doctor about the procedure to be used.
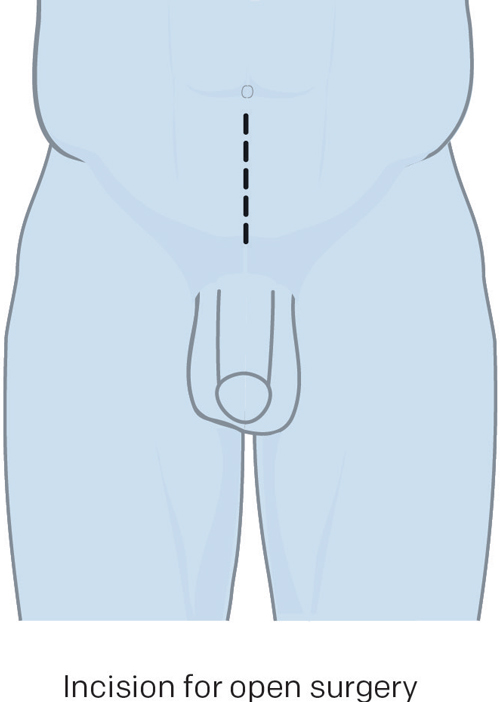
Instead of a single incision, five or six small ones (about one centimetre in length) are made in the lower abdomen. Long, slim surgical instruments are inserted through these incisions to guide the operation.
A telescopic instrument called a laparoscope is inserted into the abdomen through a small incision at the belly button.
A camera attached to the laparoscope allows surgeons to see inside the abdomen and perform the surgery without having to make a large incision.
While this technique generally shortens recovery time, it is not proven to be any more effective than open surgery performed by an experienced surgeon.
This technique runs the same risks for incontinence and erectile problems as open surgery.
Laparoscopic prostatectomies have not gained widespread acceptance because they are technically difficult to perform even in the hands of skilled laparoscopic surgeons. Specialized training and equipment are required.
In recent years, robotic surgery has developed and become increasingly popular. As the learning curve is faster for robotic surgery than for laparoscopy, this type of surgery is more and more widely used by urological surgeons.
The movements of robotic instruments are intuitive, and the surgeon has a 3D‑view of the prostate. In addition, robotic instruments have articulated tips which mimic human wrist movements.
While this technique generally shortens recovery time, it has not been proven to be any more effective than hand-assisted laparoscopies or open surgeries performed by an experienced surgeon.
Unfortunately, patients still run the same risk for incontinence and erectile problems as in open surgery.
There are also economic considerations with robotic surgery—specialized training and equipment are required—and only centres with a high volume of cases can offer this technique.
We know that you are faced with a choice between several surgical techniques. Which one is the best? We’re not in a position to say yet. The most important factors are the skill and experience of the surgeon rather than the method used. Therefore, we suggest you talk to your surgeon about his or her experience with the different techniques available. We will discuss this subject a little further on in this page.
Surrounding the prostate are bundles of nerves responsible for erections. When the surgeon removes your prostate, he will try to save these nerves. This is known as “nerve-sparing” surgery.
Whether or not the nerves can be spared depends on how close the cancer is to the nerves. It is difficult for the surgeon to know before surgery if the nerves can be spared. The decision to spare nerves is made once the prostate and the tumour can be seen during surgery.
Nerve-sparing surgery is more successful with early stage prostate cancer and for younger, sexually active men.
 Advantages of radical surgery
Advantages of radical surgeryA radical prostatectomy is a major operation, and as with all major operations, there are short-, medium-, and long-term risks and complications. It does not affect all men in the same way—it all depends on the surgery and your general state of health.
Complications during surgery are rare, but may include:
Post-operative complications, once you have returned home, may include:
The most common problems associated with radical prostatectomy are:
To learn more about incontinence or erectile dysfunction, see our section on side effects.
The success of the surgery and the risk of side effects depend on the experience and skill of your surgeon. Your surgeon should be able to tell you how many operations he has performed, the success rate of these surgeries, and the rate of side effects in his patients.
Surgeons, who are in the operating room on a regular basis (ex. 3 times a month) or perform at least 20 radical prostatectomies a year, ideally more than 35 a year, have better outcomes including a lower rate of side effects.
It is important to note it’s not the number of patients operated on that counts, but the experience of the surgeon. In this regard, ask your surgeon if they can put you in touch with one of their patients. There are also websites where patients give their opinions about doctors. Be careful, as you may become more confused about your surgeon’s skills, as opinions may be completely different from one patient to the next.
If your surgeon has taken the time to talk to you, answer your questions regarding his success rate, his failures, and time spent in the operating room and has given you confidence in his abilities, it is a safe bet that you are in very good hands. And it is definitely the hands of the surgeon that make the difference, regardless of whether the surgery is conventional (open) or robotic.
 Your doctor has offered you radical surgery to treat your prostate cancer? This section describes this treatment and the precautions to be taken to ensure that everything goes as smoothly as possible.
Your doctor has offered you radical surgery to treat your prostate cancer? This section describes this treatment and the precautions to be taken to ensure that everything goes as smoothly as possible.
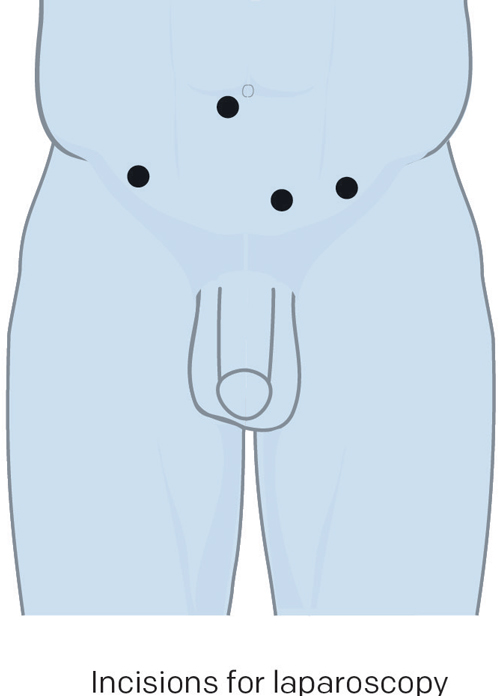
To familiarize you with medical language, here is a brief description of structures that make up the male reproductive system.
Bladder: The muscular sac-like organ in which urine is collected and stored in the body.
Prostate: The gland located just below the bladder that surrounds the urethra. It secretes fluids that mix with sperm cells to form semen.
Rectum: The terminal section of the large intestine.
Sphincter: Small muscle located at the opening between the bladder and the prostate. The sphincter prevents urine from leaking out of the bladder—controlling urinary continence.
Seminal vesicles: Small pouches that store the sperm produced by the prostate.
Urethra: The tube that carries urine from the bladder and sperm secreted by the genital glands out through the penis.
Testicles: The two glands located inside the scrotum that form sperm cells and produce testosterone (male hormone).
You will be hospitalized either on the day of or the day before your operation and will stay for anywhere from 24 hours to a few days, if there are no complications.
Two to 4 hours. If your surgeon tells you that he or she can perform this procedure in less than two hours, get a second opinion.
You will be given general anesthesia or spinal anesthesia (or an epidural like those given to women in labour) so you won’t feel a thing. During the operation, the surgeon will remove your:
While you are still under anesthesia, a urinary catheter will be inserted through your penis to drain urine from your bladder during your healing process. Your catheter will remain in place for 1–2 weeks after your surgery.
In the days following your operation, your prostate, seminal vesicles, and removed tissues will be analyzed by a pathologist. This will allow your surgeon to identify the exact size and nature of your tumour.
Your PSA level should drop to an undetectable level (0) once your prostate has been removed.
 If you are well-prepared, your post-surgery recovery will be less trying than expected. Being well-prepared will help you recover more quickly and be less stressed. By reading the following, you will know exactly what is waiting for you.
If you are well-prepared, your post-surgery recovery will be less trying than expected. Being well-prepared will help you recover more quickly and be less stressed. By reading the following, you will know exactly what is waiting for you.
It is important to move to stay healthy, even if you have prostate cancer. Consequently, if you’re already practicing a regular activity, you should continue doing it until the surgery. If this is not the case, it’s never too late to add exercise to your daily routine; even if it’s at a lower intensity.
Even taking a short 15–30 minute walk can be beneficial.
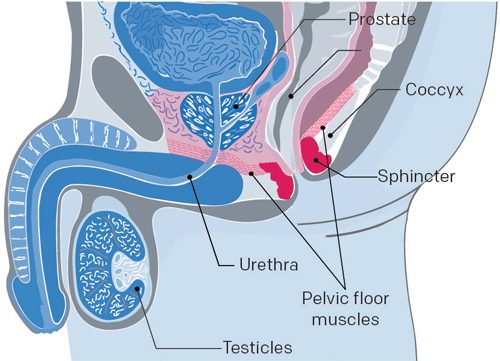
Doing pelvic floor muscle exercises are extremely effective in reducing incontinence after a radical prostatectomy. You should start doing these exercises before your operation and continue doing them after the withdrawal of the catheter. You should see an improvement after 5–6 weeks of regular exercise.
Sit, stand, or lie down with your knees slightly apart—imagine that you’re holding in your urine or bowel movement. Contract the muscles you would use in this situation.
To know if you’re contracting the right muscles, look at your penis—it should tighten and contract inwards. You should also feel the rectum muscles —the muscles you use to hold in your gas and bowel movements—tighten and contract.
When your muscles are stronger and you are leaking less, you can reduce the exercises to 10 contractions, two or three times a week. Remember that every man is different.
Physiotherapy in perineal rehabilitation is recommended by doctors and aims to strengthen the pelvic floor muscles in order to contribute to a better closure of the urethra. Your physiotherapist, an expert in perineal rehabilitation (important), can advise you on good hydration habits (water resources), constipation control, control techniques for urinary problems and the integration of good perineal contractions at the appropriate times.
You won’t have any choice but to tell your employer. Planning your time off and your return to work is important for both your recovery and peace of mind. If you work, you should address the subject as soon as possible. You should be prepared to be away from work.
After 6 weeks, you may be able to work full-time. The duration of your sick leave will vary depending on the speed of your recovery and the type of work you do.
If you have private insurance, talk to your insurance provider or your company’s human resources department to plan for your absence and minimize your stress.
Even if it’s stressful, it is recommended that you stop smoking 6 weeks before your surgery in order to reduce the risks of lung, healing, and infection problems. If needed, your doctor may prescribe medication to help you.
Alcohol can also interact with medication. This is why it is recommended to reduce its consumption and not drink in the 24 hours before surgery.
A healthy and balanced diet will also help you to recover quickly after the surgery. Energy, proteins, vitamins, and minerals that you get from your food can help fight against these infections and help contribute to your healing.
If medication is prescribed by your doctor or cardiologist, check with them before you stop taking it. Medication containing acetylsalicylic acid (Aspirin) can increase the risk of bleeding. You will need to stop taking it 7–14 days before the operation.
If you are taking this medication to relieve pain, opt for medication containing acetaminophen (Tylenol).
As some natural products can interact with medication given to you at the hospital, it is better to avoid them. If needed, discuss it with your urologist first.
After surgery, you won’t necessarily have the energy to prepare your meals, complete your daily tasks, or even bathe yourself. If possible, prepare a few meals before the surgery and freeze them. You can then easily reheat them during your recovery.
Ask family and friends to help you with certain tasks if you need it.
If there are no complications, you will be able to leave the hospital 1 to 4 days after the operation if everything goes smoothly. However, it could be stressful for you and you won’t be able to drive yourself home. It would be much better if you had someone to take you home. It is also important to note that after your surgery, you should not drive for at least two weeks.
 Before undergoing surgery, you may be required to attend a pre-admission session at your hospital. You will sign a discharge of liability releasing your surgeon and the hospital from any responsibility of risks during surgery. This discharge is mandatory for all surgeries.
Before undergoing surgery, you may be required to attend a pre-admission session at your hospital. You will sign a discharge of liability releasing your surgeon and the hospital from any responsibility of risks during surgery. This discharge is mandatory for all surgeries.
All examinations listed above are done on an outpatient basis a few days or weeks before the operation.
Usually, the meeting with your surgeon has already taken place. If you have other medical problems after your tests, you may be referred to another medical specialist before your surgery.
The hospital staff will also explain the admission procedure to you and give you any instructions you need to follow before the surgery; such as restrictions on food and beverages after midnight. Find out about the facilities the hospital offers for storing your personal effects.
Blood transfusions are rarely necessary, because in general, you will not lose much blood. Nevertheless, as a precaution, some hospitals ask their patients to provide some of their own blood before the operation. This way, if you need a blood transfusion during or after surgery, your own blood will be used. This is known as an “autologous donation”.
It is discarded if it is not used as hospitals are not authorized to keep it or use it for other patients.
You may be required to take a laxative the evening before and use an enema the morning of the operation to ensure that your bowel is clear of fecal matter. One thing is for sure, no food or liquids in the 8 hours before the operation.
Be sure to have an in-depth discussion with your urologist about the implications of the surgery, the impact it will have on the quality of your life and sexuality, and the tools available that can help you deal with it all. Don’t be afraid of reconsidering or discussing your options again if you are uncertain.
It is important to have a clear understanding of the prescriptions your urologist will prescribe for you to take when you get home. Your pharmacists can also give you advice, but you should first talk to your urologist.
Make sure that you also understand how to resume your Kegel exercises.
Finally, ask about penile rehabilitation and the early use of prescription drugs—erectile dysfunction medications in particular—after surgery to help the penis quickly regain erectile function. Please note that this approach is not universally accepted due to the lack of research on the subject. However, you can discuss the subject with your doctor.
If your urologist doesn’t bring up the subject during your preoperative visit or follow-up appointment, don’t hesitate to it up yourself.
The day before your surgery, the Admitting Department will call you to tell you when to arrive at the hospital. You should arrive 2–3 hours before your surgery. The time of your surgery is not final—your surgery could take place before or after the scheduled time.
If you are sick, call your surgeon’s office as soon as possible. If you can’t reach your surgeon, call your hospital’s admitting department.
If your surgeon is late or cancels due to an emergency, your surgeon will postpone your surgery and reschedule it for as soon as possible.
The evening before the surgery
The morning of the surgery
Leave any valuable objects, credit cards, and jewellery at home. The hospital is not responsible for objects that are lost or stolen. Some hospitals will offer you a locker for your personal effects but you may be responsible for bringing your own lock. Find out about facilities your hospital offers for storing your personal effects.
You won’t have the time to read because you will be asked to move, eat, drink, urinate, move again, manage your pain, and deal with physical shock. Ideally, if everything goes well, you will be released from the hospital after 24 hours.
 The day of the operation
The day of the operationYour family and friends can wait for you in the room or in the cafeteria. ATMs are usually available in most hospital centres.
You will be given fluids intravenously until you are able to drink and eat normally. N.B.: When you walk, you will need to push the IV pole with the hand that is not connected to the IV.
A drain, such as a Jackson-Pratt tube, will be installed in you. The drain is a special tube that prevents blood and fluid from building up inside your abdomen. It consists of two major parts: a flexible tube and a collection bulb. Most patients do not return home with their drain but it is possible. If this is the case, you will be instructed on how to take care of it once you get home.
You will come back from the operating room with a catheter, a tube inserted into your penis called a urinary catheter, which will drain urine from your bladder to a collection bag. You will leave the hospital with your catheter. It is possible for your urine to be tinged with blood—don’t worry.
You might have small tubes in your nostrils to give you oxygen. You will have a small clip on your finger to measure your blood oxygen levels. This is called pulse oximetry. The nurse will adjust the amount of oxygen given to you based on the results and will stop giving you oxygen when you no longer need it.
 After your surgery, you will wake up in the post-anesthesia care unit, also known as the recovery room. This is a quiet place where patients are carefully monitored. You will stay in recovery for several hours.
After your surgery, you will wake up in the post-anesthesia care unit, also known as the recovery room. This is a quiet place where patients are carefully monitored. You will stay in recovery for several hours.
When you are ready, you will be taken to your room. Visitors are not allowed in the recovery room, unless you stay overnight. Your family will be able to visit you when you are in your room.
It is normal to feel pain after your surgery. It will feel like a burning or tightening sensation in the area around your incisions. The pain is stronger in the first 24–48 hours and will then gradually decrease.
It is important to control your pain because it will help you to:
Your nurse may ask you to rate the level of your pain on a scale from 0 to 10. Level 0 means you feel no pain and 10 is the worst pain you can imagine. The staff will want to keep your pain under 4 out of 10. If you are in pain, you need to tell them.
The most common possible side effects of pain medication are:
If you experience any of these symptoms, tell your nurse and they will help you. Remember, it is very important that you not wait until the pain is intense to ask for sedatives. If you do, the medication will be less effective and will delay pain relief.
It is important to move around in your bed to avoid pneumonia, blood clots, and loss of muscular strength. Start the following exercises as soon as you wake up and continue doing them for as long as you are in the hospital.
Regardless of the type of stockings, by squeezing the legs a little, blood circulation is improved which prevents blood clots. You may be asked to wear them until you can walk normally. If you don’t have socks, you will be asked to move around quickly.
You will be encouraged to change positions and get up frequently. You will slowly progress through the following activities:
These exercises help blood circulation in your legs. While you are awake, repeat each exercise 4–5 times every half-hour.
These exercises will help you breathe deeply to avoid lung problems, such as pneumonia. They can be done with or without a spirometer (a device that allows you to see how much air you are breathing and watch your breathing improve). You will be shown how to do them.
For example, without the device, in a sitting or half‑sitting, place a hand on your and the other on your chest, then:
Repeat 8–10 times every hour. These activities help prevent circulatory (phlebitis) and pulmonary (pneumonia) complications. Being active promotes the evacuation of intestinal gas and decreases abdominal bloating.
You will leave the hospital with a catheter in your ureter and a collection bulb attached to your thigh. This apparatus is a little uncomfortable, but it’s invisible under clothing so it won’t be embarrassing. You will also have a drainage bag to use at night.
Before you leave, the nurse will teach you how to take proper care of your catheter and will make an appointment with your CLSC to have it removed at the prescribed time. This procedure is painless and lasts only a few seconds.
If you have surgical staples, arrangements will be made with your CLSC to have them removed seven days after your surgery. Butterfly closures can be used to hold the edges of your wound together.
If the surgeon used absorbable sutures—also known as dissolvable stitches—to close the wound, they will disappear on their own after 4–6 weeks. Keep the butterfly closures on for 15 days after the operation.
You will receive an appointment for a follow-up with one of the members of your urology team about 1 month to 6 weeks after your surgery.
You should receive a document summarizing your care. The document should include instructions for you to follow upon your return home and the telephone contact information of your surgeon and healthcare team should you have any concerns.
Some patients may need an injection of low molecular weight heparin for a month to prevent phlebitis. If this is the case, the procedure will be explained to you.
 Your recovery
Your recovery
You will have 2 drainage bags and a catheter stabilizer. The catheter stabilizer keeps the urinary tube in place and keeps it hooked to your leg. The small bag is for day and the bigger one is for night.
You should clean your bags every day. You can use the 2 drainage bags for a maximum of 1 month. You must then buy new ones. They are available in most medical supply stores.
Resume your Kegel exercises and develop good habits to manage urinary incontinence:

The Jackson-Pratt tube is connected to a bulb-shaped container that looks like a grenade. This container collects the fluid that drains from the incision and helps healing.
At first, the liquid might be tinged with blood. After a few days, there will be less fluid and it will become a clear yellow.
(Inform your surgeon and local CLSC)
(Inform your surgeon and local CLSC)
(Inform your surgeon or the urologist on duty)
(Go to the Emergency room and inform your surgeon or the urologist on duty)
(Go to the Emergency room without delay)
(Go to the Emergency room and inform your local CLSC)
(Go to the Emergency room without delay)
 The importance of follow-ups
The importance of follow-upsIf you need a medical certificate, don’t forget to ask your surgeon directly at least the day before your hospital stay.
You should see your urologist 4–6 weeks after you are discharged from the hospital. After this first appointment, you will see your urologist at regular intervals (3–6 months). If everything goes well, after 5 years in remission, follow-ups will become annual.
It is impossible to estimate the average success rate of radical surgery.
Your urologist will do a PSA test every time since this test is the best predictor for the risk of recurrence of prostate cancer. A digital rectal exam may also be performed sometimes.
After the operation, the PSA level should be undetectable (0) since there is no more prostate to produce antigens. At each medical appointment, your urologist will check 3 parameters:
If the PSA level starts to climb, the doctor will monitor how much time it takes to double. The shorter these periods are, the greater the risk of recurrence and the more aggressive the recurrence will be. For example, the PSA level that starts to increase eight months after the operation and that doubles in six months is much more worrisome than a PSA level that starts to climb three years after surgery and takes a year to double.
If necessary, radiation therapy and/or hormone therapy may be prescribed.
After five years without recurrence, you are considered to be in remission and the risk of recurrence is very low.
 The most common problems associated with radical prostatectomies are urinary incontinence, erectile dysfunction, and stenosis (narrowing) of the bladder neck.
The most common problems associated with radical prostatectomies are urinary incontinence, erectile dysfunction, and stenosis (narrowing) of the bladder neck.
After the surgery, practically every man experiences a transitory period of urinary incontinence. This period can last for several weeks up to a few months (average 3 to 6 months). For some men, patience will be required, since recovery may take longer (6 to 9 months) and even up to 2 years. It varies from one person to the next depending on the degree of their disease, their age, and their state of health. In most cases, urinary incontinence disappears with time and with specific exercises such as Kegels.
In a few cases, urinary incontinence can be permanent and may require a surgical implant if you are a good candidate for it.
The suture between the bladder and urethra can scar, causing a fibrosis and a narrowing of the urethra, in less than 5% of cases. This can make urinating difficult (weak urine stream and incontinence) and, in some cases, painful. This problem can easily be corrected naturally with dilation (widening).
A certain percentage of men regain erectile function 6–36 months after surgery. The speed with which their sexual function improves depends on sexual function before the operation, age, general state of health, and preservation of erectile nerves during surgery.
In some men, the surgeon is unable to save the nerves and there is a possibility of the erectile dysfunction persisting without treatment.
Treatments include oral medication such as tadalafil, sildenafil, and vardenafil; the MUSE pellet; penile injections; vacuum pumps; or surgical penile implants.
It is recommended that you do not remain sexually inactive. Penile rehabilitation, to ensure that your penis has a satisfactory erection, is extremely important after surgery. The best thing to do is to discuss it with your urologist before your surgery.
After this type of operation, you will no longer have an ejaculation; the seminal vesicles and prostate that produce seminal fluid (semen) have been removed. This is what we call a dry orgasm. The absence of sperm will result in infertility.
Your libido and orgasms will still be there. There may be a small amount of urine that leaks out during intercourse because the sphincters relax. This is why it is better to urinate before having sex.
Some men find that radical surgery shortens their penis. It seems that this is not really the case. This impression may come from the fact that when you go a long time without having an erection, the penis can retract from lack of blood flow.
To avoid fibrosis—the hardening of penile tissues caused by the lack of blood and oxygen—men are encouraged to have erections, with or without treatment, as soon after surgery as possible. This will speed up the recovery process and your ability to have an erection while reducing the risk of your penis shortening.
To learn more about incontinence or erectile dysfunction, take a look at our section on side effects.
 Give yourself time
Give yourself timeAfter a radical prostatectomy, many men have mood swings and feelings of sadness, happiness, and fear.
They also stressed the need to continue having intimate relations with their partner despite their inability to have full intercourse. Touching, kissing, holding hands, walking together, talking at length, and just being together can be deeply satisfying and help you recover.
Orgasms will return in due time. We recommend that you talk openly with your partner about your thoughts and concerns and with your urologist.
Things to remember when you are ready to resume sexual activities
Here are some questions you can ask members of the health care team about surgery. It may be useful to bring this list to your next doctor’s appointment to write the answers.
You have questions or concerns? Don’t hesitate. Contact us at 1-855-899-2873 to discuss with one of our nurses specialized in uro-oncology. They are there to listen, support and answer your questions, and those of your family or your loved ones. It’s simple and free, like all of our other services.
Also take the time to visit each of our pages on this website, as well as our YouTube channel, in order to get familiar with the disease, our expert lectures, our section on available resources, the support that is offered to you, our events and ways to get involved to advance the cause.
Pages that might interest you
Want to know more? Just click on one of the links below.
The latest PROCURE news that might interest you
Every week we publish a blog article. Here are some we have chosen for you.
The medical content and editorial team at PROCURE
Our team is composed of urologists, and nurses certified in uro-oncology with a deep knowledge of prostate cancer and other diseases related to the genitourinary system. Meet our staff by clicking here.
Last medical and editorial review: September 2023
Written by PROCURE. © All rights reserved