The Gleason classification system is the grading system most widely used to describe the degree of aggressiveness of the prostate cancer. Prostatic tissue, obtained by biopsy, is observed under a microscope where a pathologist evaluates the cancerous tissue and compares it to normal prostate tissue. Grading is based on two components: appearance and cellular arrangement. You may have heard talk of the Gleason grade and the Gleason score. Even if the two terms both describe the aggressiveness of cancer, they are not entirely synonyms.
The pathologist uses a scale from 1 to 5, the Gleason grade, to describe the degree of abnormality in the biopsied tissue samples. The lower the number (grade 1 or 2), the more normal the cancerous cells appear and the weaker the degree of aggressiveness. Inversely, the higher the number (grade 4 or 5), the more the cancerous cells will appear to be irregular or abnormal and the more severe the degree of aggressiveness. A grade 3 is given for an intermediate condition. However, as the prostate is not homogenous throughout the gland, different grades can be assigned within the same tissue.
The normal prostate tissue consists of a structured arrangement of ducts and small glands (acini). This is an image of low grade cancer.
As the cancer cells multiply and spread, both the appearance and cellular arrangement will change. The cells change shape and begin to look less like typical prostate cells. This increase in activity also causes the cell nucleus, containing the genetic material for the maintenance, growth and reproduction of each cell, to become larger than normal. All of these changes cause the ducts and glands (acini) of the prostate to take on an irregular appearance.
These cancerous cells tend to behave very aggressively, that is to say, they spread quickly. Normal cells die off as they compete against the cancer cells for nutrients. As high-grade cancer cells continue to spread, the ducts and glands (acini) of the prostate also disappear.
In the same tissue, cancer can be more aggressive in some areas than in others (different grades coexist). Thus, to get a more accurate idea of the cancer’s spread, the pathologist assigns grades to the two most common patterns of cancer growth and adds them together to get the Gleason score. It is important to consider the order of the grades. The first number represents the most common grade and can influence your choice of treatment.
For example, the degree of aggressiveness of a cancer with grades 3 + 4 (Gleason score 7) will be lower than a cancer with grades of 4 + 3 (Gleason score 7). In cases where a predominant grade cannot be found, the pathologist will add the number to itself. For example, 4 + 4 gives a score of 8.
In theory, the Gleason score is a scale from 2 to 10, but in practice, because grades 1 and 2 are not cancer, scores are normally only between 6 and 10 (3 + 3 to 5 + 5). In general, the higher the score, the more aggressive and fast-growing it is. The Gleason score can be an important factor in your doctor’s recommendation to proceed with a radical prostatectomy.
In recent years, a new classification system has been used to assess the aggressiveness of prostate cancer: Grade Group. It simplifies classification into 5 groups.

Your urologist will analyze all the results of the tests you have done and will give a stage for your cancer depending on the size and spread of the tumour. The most commonly used method for classification is the TNM method (Tumour, Nodes [lymph nodes], and Metastases).
The T refers to the extent of the main (primary) tumor, N for whether the cancer has spread to nearby lymph nodes and M for whether the cancer has spread (metastasized) to other parts of the body.
There are 2 types of T categories for prostate cancer:
TX – Tumour cannot be assessed.
T0 – Absence of tumour in the prostate.
T1 – Tumour is small, confined to the prostate and cannot be felt during a digital rectal exam. This is a localized prostate cancer.
T2 – Tumour is contained to the prostate but can be felt during a digital rectal exam or seen on imaging (MRI). This is a localized prostate cancer.
T3 – Tumour has started to spread beyond the prostate to areas surrounding the gland. This is a locally advanced prostate cancer.
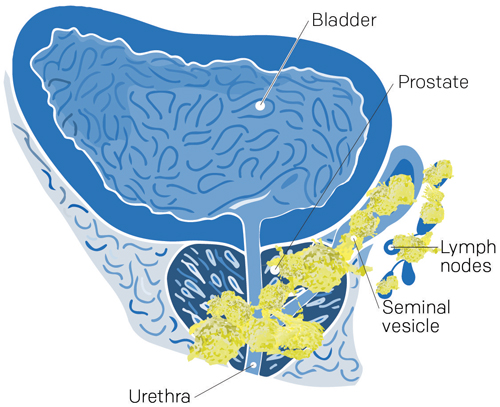
T4 – Tumour has spread beyond the prostate to nearby structures other than the seminal vesicles: rectum, urethral sphincter, bladder, and pelvic wall. This is still a locally advanced prostate cancer.
NX – Nearby lymph nodes are not measured
N0 – No cancer cells in the nearby lymph nodes.
N1 – Cancer cells present in the regional lymph nodes.
MX – No assessment of distant sites or results are inconclusive.
M0 – No distant metastases.
M1 – Distant metastases (bones, non-regional lymph nodes, liver, kidneys, lungs). This is a metastatic prostate cancer.
Grouping of TNM classification data into four stages:
Your cancer may be at low risk of spreading if:
Your cancer may be at medium risk of spreading if:
Your cancer may be at high risk of spreading if:
Localized prostate cancer is contained within the prostate, in other words, it has not spread outside of the prostate. Many localized cancers are often not very aggressive and tend to grow slowly. Because of this, chances are high that this type of cancer will not cause you any problems in your lifetime. However, some localized cancers grow more quickly than others and can spread to other parts of your body.
There is no perfect treatment for localized cancer; each treatment has its strengths and weaknesses. A radical prostatectomy (the complete removal of the prostate) or a radiation therapy treatment can be done, but simply keeping a close watch can be enough to find any cancerous growth in time. Discuss the possible courses of treatment with your urologist.
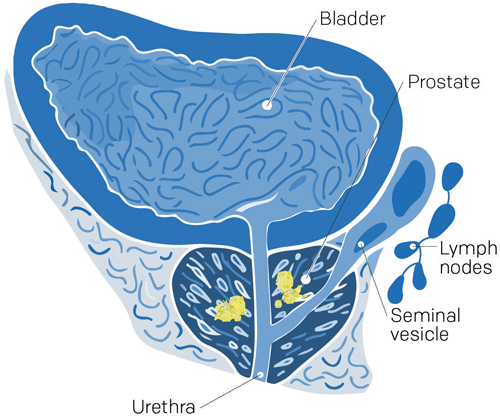
Locally advanced prostate cancer is cancer that has begun to break out of the prostate, but not too far. It may have spread beyond the boundaries of the prostate (capsule) into the neighbouring regions of the seminal vesicles, pelvic nodes, bladder, rectum, or pelvic lining.
Selecting the best treatment depends on the extent of the cancer spread:
Metastatic prostate cancer is cancer that has spread to other parts of your body — far from your prostate. Metastases originating from the prostate most often develop in the bones and lymph nodes. Bone pain, fatigue, and weight loss are all symptoms associated with advanced cancer. Advanced prostate cancer cannot be cured. There are, however, many treatments that can help to reduce symptoms and keep your cancer under control for several years. The preferred treatment for metastatic prostate cancer is hormone therapy, which aims to reduce the level of testosterone (castration), a hormone that nourishes cancer cells. It can be done surgically by removing the testicles or medically by injections or medication.
In recent years, several treatments initially used after the failure of hormone injection, such as chemotherapy and/or next-generation hormone therapy in the form of tablets, are now sometimes used when a new diagnosis of metastatic prostate cancer is made.
What 2023 research says – In patients with prostate cancer that has spread significantly throughout the body, treatment options beyond just hormone injections, such as triple therapy (standard hormone therapy, chemotherapy and oral tablets), should be discussed with your doctor. As such, here is a video clip that might interest you with Dr. Aly-Khan Lalani, Medical Oncologist at the Juravinski Cancer Centre and Assistant Professor at McMaster University, in Ontario, Canada, following the ASCO-GU scientific conference in 2023.
The recurrence of cancer can happen when some cancer cells survive after your initial treatment. Cancer can recur in the same place or it can be detected in another part of your body. The latter is also known as a metastatic recurrence. The next treatment step depends on the location of the recurrence.
Hormone therapy can keep the spread of cancer under control for a number of years. However, with time, the cancer may become castrate resistant and start to grow again. That is to say, cancer is able to replicate despite castration (the low level of testosterone). Treatments for cancers that no longer respond to hormone therapy exist, but are dependent on whether or not metastases are present.
The majority of men who have prostate cancer are diagnosed with adenocarcinoma, a malignant tumour in the glandular cells lining an organ. However, rare forms of prostate cancer also exist; the following are examples of such:
Leiomyosarcoma and rhabdomyosarcoma affect, respectively, smooth and striated prostatic muscle cells. These cancers don’t usually affect PSA levels, but often cause urinary problems. Sarcoma is found during biopsy, imaging or following a transurethral resection of the prostate used to treat urinary problems.
This cancer develops from neuroendocrine prostate cells. There are “small cell” neuroendocrine cancers and “large cell” neuroendocrine cancers that are much rarer and much less studied. Small cell carcinoma does not usually affect PSA levels and is often found following a biopsy or transurethral resection of the prostate that is used to treat urinary problems. This form of cancer tends to be aggressive, spreading to other parts of the body (metastases).
This cancer can start in the prostate, but more often than not, it starts in cancerous cells lining the urinary system (bladder, urethra, ureter, and kidney) and spreads to the prostate. This cancer is often diagnosed following a transurethral resection of the prostate.
Whether you are diagnosed with a rare form of prostate cancer or another less common type, such as ductal carcinoma, mucinous carcinoma, or signet ring carcinoma, ask your doctor to give you a detailed explanation of the cancer that you are affected by and its possible treatments.
One of the characteristics of cancer cells is their ability to spread to other parts of your body from where they originally started growing. The spread of cancer can happen in three different ways:
For the majority of cancers, places where the cancer usually spreads to are known and predictable. In the case of prostate cancer, cancer cells have a tendency to spread to the following places:
The following are a few of the serious consequences that can result from the spread of cancer: